Scapular Stability Prevents Common Shoulder Injuries
Understanding Scapular Stability Training for Upper Body Strength Enhancement
Your shoulder blades might be the most underappreciated component of upper body strength and injury prevention. While most people focus on building bigger chest muscles or stronger arms, the scapulae—those triangular bones on your upper back—serve as the foundation for nearly every upper body movement you perform. Scapular stability training for upper body strength enhancement addresses this critical yet often neglected aspect of fitness, creating a stable platform from which your arms can generate force, maintain proper positioning during movements, and protect delicate shoulder structures from injury. When these bones move correctly and maintain proper positioning, your shoulders function optimally. When scapular control breaks down, a cascade of compensation patterns emerges, leading to decreased performance, chronic pain, and eventual injury.
The scapulae don’t just sit passively on your ribcage—they glide, rotate, and stabilize through complex three-dimensional movements coordinated by seventeen muscles. This intricate system allows your shoulder joint to achieve its remarkable range of motion while maintaining stability. Without proper scapular stability training for upper body strength enhancement, even the strongest individuals develop movement dysfunctions that compromise their training progress and daily activities. Understanding how these structures work together provides the foundation for building resilient, powerful shoulders that perform optimally whether you’re reaching overhead to place items on high shelves, carrying groceries from your car, or engaging in recreational sports activities.
The Critical Role of Scapular Position in Shoulder Health
Scapular positioning directly influences shoulder joint mechanics, determining whether movements occur safely or create stress on vulnerable tissues. The scapula must upwardly rotate approximately 60 degrees during overhead movements, creating adequate space in the subacromial region where tendons of the rotator cuff pass beneath bony structures. When this rotation fails to occur properly—a condition called scapular dyskinesis—the space narrows, causing tendons to compress against bone with every overhead movement. This repetitive compression leads to inflammation, tissue damage, and eventually tears in the rotator cuff tendons. Research published in the Journal of Orthopaedic & Sports Physical Therapy demonstrates that scapular dyskinesis appears in 67-100% of individuals with shoulder pain, establishing the clear connection between scapular control and shoulder health.
Beyond rotational movement, the scapulae must maintain appropriate contact with the ribcage throughout all movements. Scapular winging—where the medial border lifts away from the ribcage—indicates weakness in the serratus anterior muscle and creates instability throughout the shoulder complex. You might notice this appearing as a prominent bone edge along your inner shoulder blade during push-up movements or when reaching forward. This positional fault redirects forces away from strong stabilizing muscles onto smaller, more vulnerable structures. The long thoracic nerve, which controls the serratus anterior, can become compressed or damaged through repetitive overhead activities, direct trauma, or poor posture, leading to progressive weakness and winging that fundamentally alters shoulder mechanics.
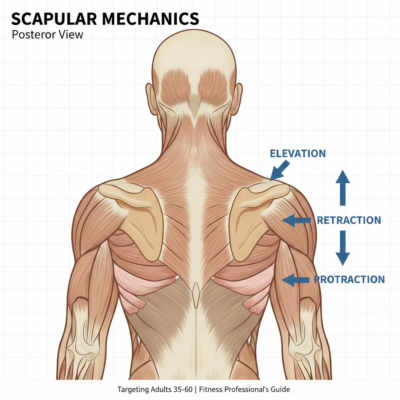
Scapular protraction and retraction must occur in proper timing and magnitude to support arm movements. During reaching activities, the scapula should protract (move around the ribcage toward the front) to extend your reach and maintain glenohumeral joint alignment. During pulling movements, retraction (drawing the shoulder blades together) provides the stable base necessary for generating force. Many people develop patterns where one movement dominates—commonly excessive protraction from prolonged computer work—creating imbalances that stress shoulder tissues during normal activities. A personal trainer can assess these movement patterns, identify specific deficits, and design corrective strategies that restore balanced scapular function.
Most Common Scapula-Related Injuries and Their Prevention
Rotator cuff impingement represents the most prevalent scapula-related shoulder injury, affecting approximately 44-65% of people experiencing shoulder pain according to the American Academy of Orthopaedic Surgeons. This condition develops when inadequate scapular upward rotation during arm elevation causes the acromion (a bony projection from the scapula) to compress rotator cuff tendons against the humeral head. Each overhead movement creates friction and inflammation in this confined space. Over time, chronic compression progresses from inflammation to partial thickness tears and eventually complete rotator cuff ruptures. Early symptoms include pain with overhead activities, night pain when lying on the affected shoulder, and clicking or catching sensations during movement. Proper scapular stability training for upper body strength enhancement addresses the root cause by ensuring adequate upward rotation occurs, creating sufficient subacromial space for tendons to glide freely.
Scapular dyskinesis itself constitutes an injury pattern characterized by abnormal scapular movement or positioning during arm motion. Clinical examination reveals asymmetry in scapular position at rest, prominence of the medial border or inferior angle during movement, or early or excessive scapular elevation during arm raising. While dyskinesis sometimes appears as an isolated condition, it frequently accompanies other shoulder pathologies, serving as both cause and consequence of shoulder dysfunction. The Scapular Assistance Test, performed by a qualified professional, determines whether manually supporting the scapula into proper position during arm elevation reduces symptoms—a positive finding indicates that scapular retraining would benefit the individual. Addressing dyskinesis through targeted stability training often resolves associated symptoms and prevents progression to more serious pathologies.
Shoulder instability conditions, including subluxations and dislocations, frequently involve scapular positioning problems that compromise the stable base required for glenohumeral joint integrity. The shoulder joint sacrifices bony stability for mobility, relying heavily on muscular control and coordination to maintain proper alignment. When scapular muscles fail to provide adequate stabilization, the humeral head translates excessively within the glenoid fossa, stretching capsular ligaments and increasing instability risk. Multidirectional instability—where the shoulder feels loose or slips out of position in multiple directions—particularly correlates with scapular control deficits. Strengthening scapular stabilizers creates the foundation upon which glenohumeral stability depends, reducing recurrence rates in individuals with instability history.
Thoracic outlet syndrome develops when nerves or blood vessels become compressed in the space between the collarbone and first rib, producing numbness, tingling, or pain radiating down the arm. Poor scapular positioning, particularly chronic depression and protraction, narrows this thoracic outlet space, compressing neurovascular structures. Individuals who spend prolonged periods with rounded shoulders and forward head posture—common among professionals working at computers—show increased susceptibility. Symptoms often worsen with overhead activities or carrying heavy bags. Scapular stability training for upper body strength enhancement restores proper scapular elevation and retraction, opening the thoracic outlet and relieving compression on affected structures.
Understanding Scapular Movement Patterns and Muscle Function
Six primary muscles attach directly to the scapula and control its position and movement on the thorax: the trapezius (upper, middle, and lower portions), serratus anterior, rhomboids (major and minor), levator scapulae, and pectoralis minor. Each muscle contributes specific actions, and their coordinated activity produces the complex scapular movements supporting shoulder function. The upper trapezius elevates the scapula, the middle trapezius retracts it, and the lower trapezius depresses and assists upward rotation. These three portions must activate in proper sequence and magnitude to control scapular positioning throughout arm movements. Imbalances between trapezius portions—particularly overactive upper trapezius combined with underactive lower trapezius—commonly appear in individuals with neck and shoulder pain.
The serratus anterior, originating from the first eight or nine ribs and attaching along the medial scapular border, performs crucial roles in scapular protraction and upward rotation. During overhead reaching, the serratus anterior works synergistically with the trapezius to rotate the scapula upward, with the serratus contributing approximately 60% of the upward rotation force. Weakness or inhibition of this muscle—whether from nerve compromise, disuse, or compensatory patterns—severely compromises overhead function and creates the scapular winging previously described. The serratus anterior also maintains scapular contact with the ribcage during pushing movements, preventing the medial border from lifting away as force transfers from the arms through the shoulder girdle to the trunk.
The rhomboids and middle trapezius work together to retract the scapulae, drawing them toward the spine. These muscles often become weak and lengthened in individuals who maintain rounded shoulder postures, creating the appearance of slouched or hunched upper backs. During rowing or pulling exercises, strong retractors provide the stable platform necessary for arms to generate maximal force. Without adequate retractor strength, the scapulae drift into protraction during pulling movements, redirecting tension away from larger back muscles onto smaller shoulder structures and diminishing exercise effectiveness. Balanced development of retractors and protractors ensures scapular positioning adapts appropriately to different movement demands.
The pectoralis minor, attaching from ribs three through five to the coracoid process of the scapula, influences scapular positioning through its actions of protraction, depression, and downward rotation. When this muscle becomes chronically shortened—common in individuals who maintain rounded shoulder postures or perform excessive pressing exercises without balanced pulling work—it holds the scapula in anterior tilt and protraction, limiting the upward rotation necessary for healthy overhead movement. Addressing pectoralis minor tightness through stretching and soft tissue work, combined with strengthening antagonistic muscles, restores balanced scapular mechanics. A personal trainer evaluates muscle length-tension relationships and designs programs addressing individual imbalance patterns.
Foundational Scapular Stability Exercises for Injury Prevention
Scapular stability training for upper body strength enhancement begins with exercises that teach conscious control of scapular positioning before progressing to movements requiring strength and coordination under load. The scapular setting exercise establishes this foundational control by having you practice moving your shoulder blades through their full range of motion against minimal resistance. Stand or sit upright with arms relaxed at your sides, then focus on drawing your shoulder blades down and together, holding this retracted and depressed position for five seconds before relaxing. Perform elevation by lifting the shoulders toward the ears, protraction by reaching the shoulder blades forward around the ribcage, and depression by pulling them downward. These movements, performed slowly with conscious attention to position, develop the mind-muscle connection essential for maintaining proper scapular control during more complex activities.
The prone scapular retraction series targets the lower and middle trapezius muscles while minimizing upper trapezius dominance. Lying face down on a bench or exercise table with your arms hanging toward the floor, initiate movement by drawing your shoulder blades together and downward without bending your elbows or shrugging your shoulders upward. Progress from this basic retraction to adding arm positions that challenge the muscles through different angles: arms at your sides (emphasizing lower trapezius), arms at ninety degrees from your body (targeting middle trapezius), and arms overhead in a Y-position (challenging both portions through their full range). Hold each retraction for three to five seconds, focusing on smooth, controlled movement rather than speed or repetition count. These exercises appear deceptively simple but prove remarkably challenging when performed with proper technique, often revealing significant weakness in these critical stabilizing muscles.
Wall slides develop coordinated scapular upward rotation and protraction while teaching proper overhead movement mechanics. Stand with your back against a wall, feet approximately six inches away from the base. Position your arms against the wall with elbows bent at ninety degrees and upper arms parallel to the floor. Maintaining contact between your arms and the wall throughout the movement, slowly slide your hands upward toward full overhead position, focusing on allowing your shoulder blades to rotate upward naturally as your arms rise. Lower with control to the starting position. Many people initially struggle to keep their arms against the wall during this movement—a clear indication of limited scapular upward rotation or thoracic spine mobility. Performed correctly, wall slides retrain the nervous system to coordinate proper scapular-humeral rhythm during overhead activities.
The bear position scapular push-up strengthens the serratus anterior while teaching scapular protraction and retraction in a weight-bearing position. Begin in a quadruped position on hands and knees, then lift your knees approximately two inches off the floor while maintaining a neutral spine position. Without bending your elbows or allowing your hips to move, allow your shoulder blades to draw together (retraction) so your chest sinks slightly between your shoulders, then actively press through your hands to separate the shoulder blades (protraction), pushing your upper back toward the ceiling. This subtle movement—typically only two to three inches of vertical displacement—specifically targets scapular muscles without involving the larger chest and arm muscles that often dominate pushing exercises. Focus on the quality of scapular movement rather than range of motion, gradually increasing repetitions as control improves.
Progressive Loading Strategies for Scapular Strength Development
Once foundational control develops, scapular stability training for upper body strength enhancement progresses to exercises incorporating external resistance and functional movement patterns. Resistance band face pulls effectively strengthen the middle and lower trapezius, rhomboids, and posterior deltoid while reinforcing proper scapular retraction mechanics. Attach a resistance band at approximately chest height, grasp the ends with both hands, and step back to create tension. Begin with arms extended forward, then pull the band toward your face by driving your elbows back and outward, simultaneously retracting your shoulder blades. The movement should finish with your hands beside your ears, elbows pulled behind your torso, and shoulder blades fully retracted. Hold this position briefly, focusing on squeezing the shoulder blades together, then return with control to the starting position. Perform higher repetitions (twelve to twenty per set) with moderate resistance to develop muscular endurance in these postural muscles.
Landmine press variations challenge scapular stability while developing pressing strength through natural movement arcs. Position a barbell in a landmine attachment or secured in a corner, load one end with appropriate weight, and stand facing away from the anchor point while holding the loaded end at shoulder height. Press the bar forward and upward, allowing your scapula to naturally protract as you reach full arm extension. This protraction differs from the retracted position maintained during bench pressing, training the scapula to move appropriately during different pressing actions. The angled bar path reduces shoulder strain compared to vertical overhead pressing while still challenging scapular control through a significant range of motion. Perform both bilateral (two-hand) and unilateral (single-arm) variations to develop balanced strength and address asymmetries.
Turkish get-ups represent a comprehensive movement challenging scapular stability throughout complex transitions between lying, sitting, kneeling, and standing positions. Begin lying on your back with a kettlebell or dumbbell held in your right hand, arm extended vertically above your shoulder. Throughout the entire movement sequence, maintain your eyes on the weight and keep your shoulder packed (scapula stabilized against your ribcage). Progress through the movement stages—rolling to your left elbow, pressing to your left hand, bridging your hips, sweeping your left leg through to a kneeling position, and standing—before reversing the sequence to return to the floor. This exercise demands constant scapular adjustments to maintain shoulder stability as body position changes, developing the dynamic stability required for real-world activities. A personal trainer provides essential guidance when learning this complex movement, ensuring proper progression and technique.
Serratus punches, performed in various positions, specifically target this crucial upward rotation muscle. The standing cable serratus punch begins with a resistance band or cable attachment positioned at chest height. Stand sideways to the anchor point, grasping the handle with the inside hand, arm extended forward. Maintaining arm extension throughout the movement, protract your scapula by reaching forward an additional three to four inches, then retract to the starting position. The movement occurs entirely at the shoulder blade, not the elbow or shoulder joint. Progress to performing serratus punches in a plank position, where you maintain a rigid body position with hands on the floor while allowing the shoulder blades to retract (chest sinks between shoulders) then protract (push upper back toward ceiling). This loaded position significantly increases serratus activation while developing the integration between scapular and core stability.
Integrating Scapular Stability Into Compound Movement Patterns
Scapular stability training for upper body strength enhancement achieves maximum effectiveness when integrated into the compound movements you perform regularly rather than treated as isolated corrective exercise. During bench press and push-up variations, maintaining proper scapular positioning protects shoulder structures while maximizing force production. Before descending into the press, actively retract and depress your shoulder blades, creating a stable platform against the bench or floor. Maintain this packed shoulder position throughout the movement rather than allowing the shoulder blades to protract or elevate as fatigue develops. This stable base allows you to generate greater pressing force while reducing strain on the anterior shoulder capsule and reducing impingement risk.
Overhead pressing movements demand precise scapular-humeral rhythm, with the scapulae upwardly rotating as the arms rise overhead. Unlike bench pressing, where scapular retraction remains constant, proper overhead pressing requires allowing the shoulder blades to move naturally through their complete range. Begin with shoulders down and back, then as you press upward, allow the scapulae to rotate upward and the shoulder blades to protract slightly as you reach full extension. Many lifters attempt to maintain retracted shoulders throughout overhead pressing, which actually limits healthy scapular movement and increases impingement risk. Focus on actively shrugging upward at the top of the press, ensuring full scapular elevation and upward rotation. This complete range of scapular motion maintains subacromial space and distributes stress appropriately across shoulder structures.
Rowing exercises provide excellent opportunities to develop and reinforce scapular retraction strength while building upper back musculature. Whether performing bent-over barbell rows, single-arm dumbbell rows, or cable rowing variations, initiate every repetition by retracting the scapula before bending the elbow. This sequence ensures that scapular muscles perform their primary role rather than allowing the arms to dominate the movement. Pull the weight until your shoulder blade reaches full retraction, hold briefly while consciously squeezing the muscles between your shoulder blades, then lower with control while maintaining scapular control throughout the descent. This intentional approach to rowing transforms these exercises into powerful scapular strength builders rather than simply arm exercises.
Pull-ups and chin-ups challenge scapular depression strength through their unique demands of supporting and moving body weight against gravity. Before pulling yourself upward, establish scapular depression by actively drawing your shoulder blades down, creating space between your shoulders and ears. Maintain this depression throughout the ascending and descending phases. Many people lose scapular control at the bottom of pull-ups, allowing the shoulder blades to elevate and the shoulders to shrug toward the ears—a position that increases shoulder stress and reduces exercise effectiveness. Performing scapular pull-ups (also called scapular shrugs) as a separate exercise develops this depression strength. Hang from the bar with arms fully extended, then without bending your elbows, depress your scapulae to lift your body one to two inches. This isolated scapular movement strengthens the depressors and teaches the proper mechanics for full pull-up performance.
Assessment and Correction of Scapular Dysfunction Patterns
Identifying your specific scapular dysfunction patterns enables targeted correction strategies rather than generic exercise prescription. The lateral scapular slide test provides objective measurement of scapular positioning asymmetry. Standing with arms relaxed at your sides, a trained professional measures the distance from the spine to the inferior angle of each scapula. Measurements repeat with hands on hips (slight abduction) and with arms elevated to ninety degrees. Side-to-side differences exceeding one centimeter suggest scapular positioning asymmetry requiring attention. While some asymmetry appears normal, particularly in individuals who perform asymmetrical activities or sports, excessive differences indicate control deficits predisposing to injury.
The scapular dyskinesis test evaluates movement quality during dynamic arm motion. A trained observer watches scapular movement from behind as you perform five to ten repetitions of weighted shoulder flexion (raising arms forward and overhead) or abduction (raising arms to the sides). Abnormal findings include early scapular elevation, excessive or rapid movement, asymmetry between sides, or prominence of the medial border or inferior angle. Subtle dyskinesis categorized as Type I features prominence of the inferior angle, Type II shows prominence of the medial border, and Type III demonstrates excessive superior translation of the entire scapula. Each pattern suggests specific muscle imbalances requiring different corrective approaches. A personal trainer trained in movement assessment identifies these patterns and develops appropriate intervention strategies.
Muscle length testing reveals tightness patterns contributing to scapular dysfunction. Pectoralis minor tightness, assessed through measuring the distance from the examination table to the posterior shoulder while lying supine, commonly restricts scapular movement. Latissimus dorsi tightness, evaluated through overhead reaching range while maintaining neutral spine position, limits scapular upward rotation. Levator scapulae and upper trapezius tightness, tested through side-bending and rotation movements, creates elevated and protracted resting scapular positions. Identifying and addressing specific tightness patterns through targeted stretching and soft tissue work complements strengthening exercises, creating balanced length-tension relationships that support optimal scapular mechanics.
Strength testing of individual scapular muscles guides exercise selection and progression. Manual muscle testing performed by qualified professionals isolates specific muscles to identify weakness patterns. The middle trapezius test positions you prone with your arm abducted to ninety degrees and externally rotated. You lift your arm against gravity and resistance while the examiner assesses strength. Serratus anterior strength testing occurs in various positions, including the wall push-up plus position where scapular protraction occurs against body weight resistance. Comparing strength between muscles and sides reveals imbalances requiring prioritized attention. Rather than performing generic scapular exercises, testing directs training toward specific deficits, accelerating correction and improving outcomes.
Professional Guidance and Long-Term Scapular Health Strategies
Working with a qualified personal trainer provides essential guidance for developing proper scapular control and preventing the common mistakes that limit progress or create new problems. Many individuals struggle to feel scapular muscles working during exercises, instead relying on larger, more familiar muscles to dominate movements. A skilled trainer provides tactile cueing—placing hands on your scapula or surrounding muscles—that helps you understand proper movement and muscle activation. This external feedback accelerates learning and ensures exercises target intended muscles rather than reinforcing existing dysfunction patterns. The investment in professional instruction prevents months of ineffective training and reduces injury risk during the learning process.
Scapular stability training for upper body strength enhancement requires consistent attention rather than a brief corrective phase before returning to previous training patterns. The muscles controlling scapular position respond to the demands you place on them daily—both during structured exercise and throughout regular activities. Maintaining awareness of shoulder blade position during computer work, driving, carrying objects, and other daily activities reinforces the patterns developed during formal training. Periodically reassessing scapular control and adjusting your program as strength develops or activities change ensures continued progress. Many people benefit from including scapular-focused exercises in every upper body training session rather than treating them as occasional supplementary work.
Addressing scapular stability creates improvements extending beyond injury prevention to enhance performance in various activities. Golfers develop more consistent, powerful swings through improved shoulder girdle stability during rotation. Tennis players generate greater racket speed and accuracy through proper force transfer from legs through stable scapulae to the arm. Swimmers reduce shoulder pain while improving stroke efficiency through optimized scapular positioning. Even non-athletic activities—reaching overhead to retrieve items, carrying children or groceries, performing yard work—become easier and less likely to cause discomfort when scapular control supports these movements. The investment in developing scapular stability yields returns across all aspects of life requiring upper body function.
Technical Considerations for Optimal Scapular Training Adaptation
Scapular muscles predominantly contain Type I muscle fibers, which respond optimally to higher volume training with moderate loads and shorter rest periods compared to traditional strength training approaches. Research published in the Journal of Athletic Training demonstrates that scapular stabilizer muscles show greater endurance deficits than pure strength deficits in individuals with shoulder dysfunction. Programming should emphasize sets of twelve to twenty repetitions for most scapular-specific exercises, with rest periods of thirty to sixty seconds between sets. This approach develops the muscular endurance necessary for maintaining proper scapular positioning throughout prolonged activities rather than only during brief, maximal efforts.
Exercise tempo manipulation enhances scapular control development by emphasizing the eccentric (lowering) and isometric (holding) phases where many individuals demonstrate control deficits. Using a four-second eccentric phase, two-second isometric hold, and two-second concentric phase during scapular exercises—often denoted as 4-2-2 tempo—significantly increases time under tension and neural adaptation. This slower execution eliminates momentum, forcing target muscles to control movement throughout the entire range of motion. Many people discover that loads they could easily move with faster tempos become challenging when tempo control requirements increase, revealing control deficits masked by compensation patterns during faster movements.
Positional variety during scapular training addresses the three-dimensional nature of scapular control requirements. The scapula must maintain stability in standing, seated, prone, supine, side-lying, and inverted positions, each presenting unique gravitational and stability demands. Including exercises in multiple positions throughout your training week ensures comprehensive development rather than position-specific adaptations. For example, performing prone scapular retractions develops different aspects of control than standing rows, despite both involving retraction movements. The varied neural demands of different positions create more robust and transferable scapular stability applicable across diverse real-world situations.
Unilateral training reveals and addresses asymmetries often masked during bilateral exercises. Many people demonstrate significant differences in scapular control between dominant and non-dominant sides, creating imbalanced loading patterns that predispose to injury on the weaker side. Single-arm rows, presses, and carries require each shoulder to independently maintain proper scapular positioning without assistance from the opposite side. Begin unilateral exercises with your weaker side, performing a target number of repetitions with proper form, then match that same number with your stronger side rather than allowing the stronger side to perform additional repetitions. This approach gradually reduces asymmetries rather than maintaining or exacerbating existing imbalances.
Conclusion
Scapular stability training for upper body strength enhancement represents a fundamental component of comprehensive fitness programming, directly impacting both injury prevention and performance optimization across all upper body activities. The scapulae serve as the foundation upon which shoulder function depends, and addressing this foundation creates improvements extending throughout the entire upper extremity kinetic chain. Understanding common scapula-related injuries—including rotator cuff impingement, scapular dyskinesis, shoulder instability, and thoracic outlet syndrome—emphasizes the clinical importance of maintaining proper scapular control and positioning. By incorporating the foundational exercises, progressive loading strategies, and assessment techniques outlined above, you develop the stability necessary to support long-term shoulder health while building functional upper body strength that transfers to all aspects of daily life and recreational activities. Working with a qualified personal trainer ensures proper technique, appropriate progression, and individualized programming addressing your specific needs and goals, maximizing the effectiveness of your training investment while minimizing injury risk throughout your fitness journey.